
近日,《表型组学(英文)》(Phenomics)在线发表了中南大学湘雅医院吴丽莎教授团队题为“A Simpler, More Convenient and More Comfortable Approach for Treating Multiple Keratinocytic Carcinoma”的研究论文。
文末点击“阅读原文”可在线阅读文章。

扫描二维码 | 下载PDF原文
论文DOI链接:
https://doi.org/10.1007/s43657-025-00220-1
论文引用格式:
Jiang, Z., Liu, X., Peng, L. et al. A Simpler, More Convenient and More Comfortable Approach for Treating Multiple Keratinocytic Carcinoma. Phenomics (2025). https://doi.org/10.1007/s43657-025-00220-1
研究背景
角质形成细胞来源的皮肤肿瘤(Keratinocytic carcinoma,KC)既往也被称为非黑色素瘤性皮肤肿瘤(Non-melanoma skin cancer,NMSC),主要包括基底细胞癌(Basal cell carcinoma,BCC)和皮肤鳞状细胞癌(Cutaneous squamous cell carcinoma,cSCC)。多发损害在KC中较为常见,7%-30%的BCC患者和10%-20%的鲍温病(原位cSCC)患者同时存在≥2个皮损[1-2]。本研究将单一类型KC病灶≥3个和/或同时存在两种及以上KC病灶的情况定义为多发性KC。相较于单发损害的患者,多发KC患者的治疗更为棘手。当病灶位于面部、颈部等暴露部位时,在去除病灶的同时很难兼顾美观性[3]。除美观问题外,多发KC与不良预后相关。存在≥2个皮损的BCC患者中有41%会继发新病灶,多发性cSCC患者的预后亦显著劣于单发病例[4]。研究证实,多发性KC患者不仅继发皮肤肿瘤风险更高,且治疗成本显著增加[5-6]。
尽管扩大切除术适用于大多数KC,但需注意80%的KC发生于60岁以上老年人,而多发性KC患者平均年龄更大[7]。这类老年患者常存在传统手术禁忌症,如免疫抑制状态、合并抗凝治疗或全身状况差。此外,传统扩大切除术对累及眼睑、唇部、耳部等需最大限度保留正常组织的区域并不适用,因其可能破坏正常解剖结构与功能[8]。而非手术治疗(如维莫德吉、放疗、咪喹莫特、冷冻治疗等)则存在疗效不佳与高复发风险的问题。
光动力疗法(Photodynamic therapy,PDT)作为一种无创治疗技术已广泛用于治疗KC,尤其适用于多发病灶[9]。最新研究显示,通过联合刮除术、浅表削切术、激光等物理预处理方法,可显著增强光敏剂渗透性,从而提升PDT治疗难治性皮肤病的效果[10]。本研究旨在探究原位手术联合PDT治疗多发性KC的有效性及安全性,并浅析PDT治疗多发性KC的作用机制。
研究结果
本研究纳入了23位多发性KC患者,共计130处病灶接受原位手术联合PDT治疗。患者平均年龄为65.97±13.59岁,其中14位(60.9%)为男性患者。多发性光化性角化病(Actinic keratosis,AK)、BCC和鲍温病分别诊断于2位(8.7%)、10位(43.5%)和13位(56.5%)患者(1位患者为AK合并鲍温病,1位患者为BCC合并鲍温病),16位(69.6%)患者存在位于头面部的皮损。原位手术联合PDT治疗的流程如图1所示,对于可以直接缝合的KC皮损,选择原位切除;对于难以切除后缝合的、较大的KC皮损,选择原位切削。在手术处理后进行光敏剂的孵育和首次PDT治疗。此后每周进行一次PDT治疗,共计2-4次,根据皮损的具体情况确定光动力治疗的疗程数。
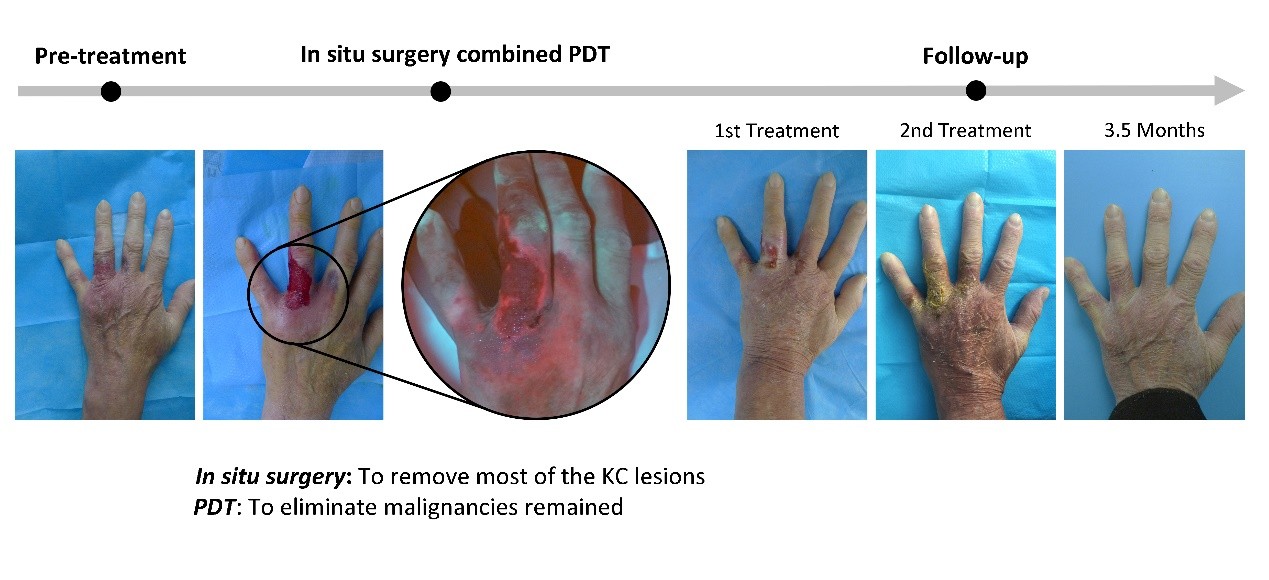
图1. 原位手术联合PDT治疗多发性KC的流程图
治疗后3月,所有经原位手术联合PDT治疗的皮损均完全响应(100%)。治疗期间,10例(43.5%)患者疼痛评分≤3分(提示轻度疼痛),平均疼痛评分为4.39分。其他不良事件包括灼热感(21.7%)、红斑(8.7%)、瘙痒(8.7%)及结痂(4.3%)。治疗前DLQI平均得分为11.91±5.07,3个月随访时显著下降至3.00±3.08(p<0.001),提示患者生活质量显著改善。随访时间16-92个月(平均35个月),仅1例结节型BCC出现局部复发,复发率为1/130(0.76%)。美容效果评估显示,14例(60.9%)患者报告“非常满意”,7例(30.4%)患者报告“满意”,2例(8.7%)患者报告“一般”,满意度平均得分4.26分(范围1-5)。
观察到有1例结节型BCC在联合治疗后20个月出现复发,为探究潜在的分子机制,我们检测了该患者复发病灶(Relapsed lesion,RL)、该患者未复发病灶(Non-relapsed lesion,NL)与其他患者NL中PDT相关分子的表达。图3a(左)显示,作为转移与进展促进因子的MMP-2在RL中表达水平最高,而同一患者NL及其他患者NL的MMP-2表达显著降低。铁死亡相关蛋白GPX4和FSP1在RL中的表达同意较NL显著升高(图2a中、右),提示MMP-2升高可能通过抑制铁死亡导致PDT治疗后预后不良。
我们继续进行体外实验验证上述猜想。采用铁死亡抑制剂Liproxstatin-1(Lip-1)联合PDT处理人cSCC A431细胞。如图2b-c所示,PDT处理后铁死亡相关基因TFRC和SLC7A11的蛋白及mRNA水平显著升高,而铁死亡标志物GPX4显著降低,表明PDT可能通过下调GPX4及上调TFRC/SLC7A11诱导A431细胞铁死亡,该效应可被Lip-1部分逆转。明胶酶谱分析显示,PDT显著增强MMP2/9活性,而Lip-1可抑制此效应(图2d)。值得注意的是,PDT虽降低MMP-2 mRNA表达,但Lip-1可恢复其抑制效果(图2e)。
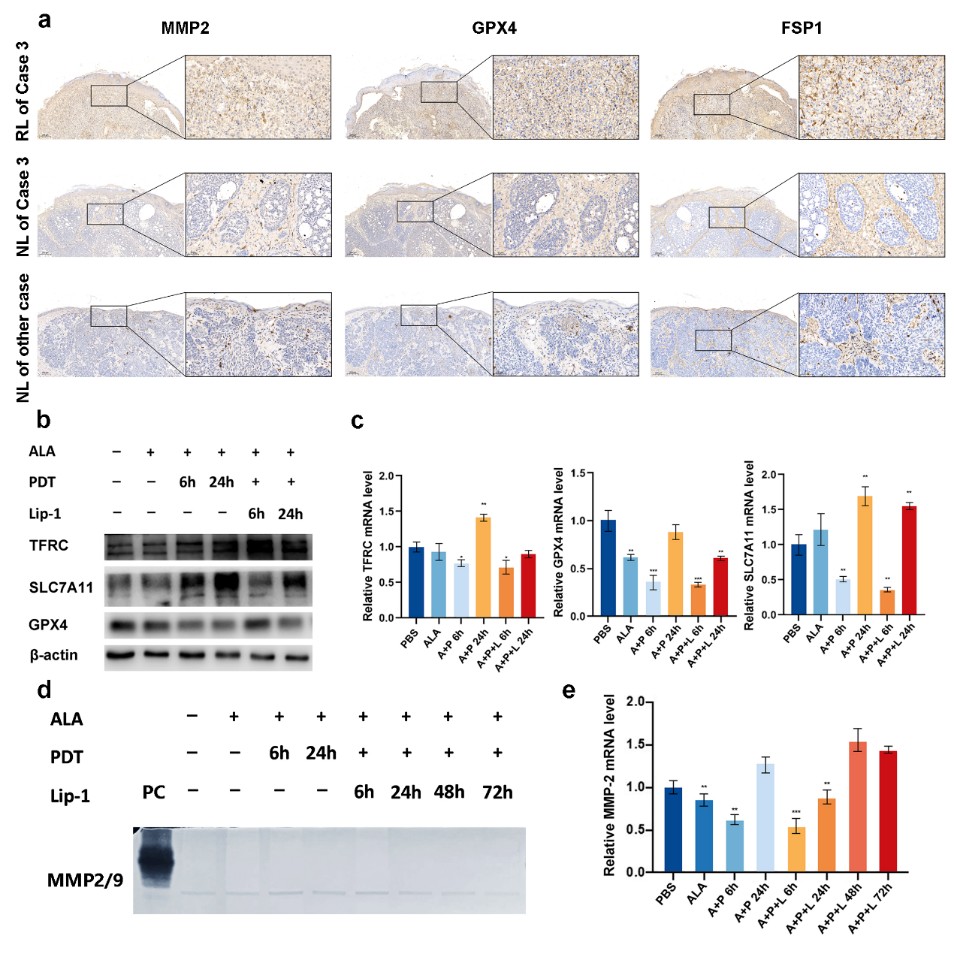
图2. 分子机制探究
讨论
本研究证实原位手术联合PDT治疗多发性KC具有较好的疗效与安全性。既往研究已报道PDT治疗多发性BCC与cSCC的案例,Mougel等报道PDT治疗多发性BCC的完全缓解率在5例患者中为85.4%[11];Girard等采用手术联合PDT治疗7例儿童多发性BCC,经3次治疗后总体反应率达78%,且所有病例均获良好美容效果[12]。本研究纳入更多病例,结果与既往研究一致,提示原位手术联合PDT方案患者耐受良好且治疗响应情况较佳。此外,我们的研究提示MMP2是PDT治疗多发性KC的潜在预后标志物,其高水平可能与治疗后较高的复发风险相关。
中南大学湘雅医院皮肤科吴丽莎教授为最后通讯作者。中南大学湘雅医院皮肤科蒋梓汐博士与刘鑫博士为共同第一作者。
Summary
Multiple lesions of keratinocytic carcinoma (KC) presenting in one patient is not rare but correlated with worse responses to current therapies. In the current study was designed to describe the safety and efficacy of combination photodynamic therapy (PDT) and surgery in situ in treating multiple KCs and investigate the prognostic biomarkers of this treatment. Twenty-three patients in two dermatological centers with multiple KCs were retrospectively enrolled. In situ surgery was performed once before the first 5‐aminolaevulinic acid PDT treatment. Complete response rate and local recurrence were assessed. Histopathological and cellular experiments were performed to search the biomarkers used to predict recurrence. The initial response rate was 100%. Local recurrence was only observed in one lesion at the followed-up 20 months. MMP-2 expression was remarkably increased in the local recurrence lesions compared to without relapsed lesions. And MMP-2 was positively correlated with PDT-induced ferroptosis-related molecules GPX4 and FSP1 expression. The expression of MMP-2 was down-regulated after PDT, and ferroptosis inhibitor prevented the decrease of MMP-2 level. In conclusion, PDT combined with in situ surgery is a potential option for treating multiple KCs patients. Elevated MMP-2 expression in KC lesions may predict the higher possibility for local recurrence after the combined therapy.
参考文献
[1] Schreuder K, Hollestein L, Nijsten TEC et al (2022) A nationwide study of the incidence and trends of first and multiple basal cell carcinomas in the Netherlands and prediction of future incidence. Br J Dermatol 186(3):476-484. https://doi.org/10.1111/bjd.20871
[2] Mohandas P, Lowden M, Varma S (2020) Bowen's disease. Bmj 368:m813. https://doi.org/10.1136/bmj.m813
[3] Lukowiak TM, Perz AM, Veerabagu SA et al (2021) Patient Quality of Life After Interpolated Flap Repair of Nasal Mohs Surgery Defects: A Multicenter Prospective Cohort Study. JAMA Dermatol 157(10):1213-1216. https://doi.org/10.1001/jamadermatol.2021.3161
[4] Kuo K, Batra P, Cho H et al (2017) Correlates of multiple basal cell carcinoma in a retrospective cohort study: Sex, histologic subtypes, and anatomic distribution. J Am Acad Dermatol 77(2):233-234.e232. https://doi.org/10.1016/j.jaad.2017.02.047
[5] Han SH, Kim SH, Kim CK et al (2020) Multiple nonmelanocytic skin cancers in multiple regions. Arch Craniofac Surg 21(3):188-192. https://doi.org/10.7181/acfs.2020.00073
[6] Gordon LG, Elliott TM, Olsen CM et al (2018) Multiplicity of skin cancers in Queensland and their cost burden to government and patients. Aust N Z J Public Health 42(1):86-91. https://doi.org/10.1111/1753-6405.12738
[7] Adachi K, Yoshida Y, Noma H et al (2018) Characteristics of multiple basal cell carcinomas: The first study on Japanese patients. J Dermatol 45(10):1187-1190. http://doi.org/10.1111/1346-8138.14576
[8] Souto EB, da Ana R, Vieira V et al (2022) Non-melanoma skin cancers: physio-pathology and role of lipid delivery systems in new chemotherapeutic treatments. Neoplasia 30:100810. https://doi.org/10.1016/j.neo.2022.100810
[9] Morton CA, Szeimies RM, Basset-Seguin N et al (2019) European Dermatology Forum guidelines on topical photodynamic therapy 2019 Part 1: treatment delivery and established indications - actinic keratoses, Bowen's disease and basal cell carcinomas. J Eur Acad Dermatol Venereol 33(12):2225-2238. https://doi.org/10.1111/jdv.16017
[10] Liu D, Zhao S, Li J et al (2021) The application of physical pretreatment in photodynamic therapy for skin diseases. Lasers Med Sci. https://doi.org/10.1007/s10103-020-03233-6
[11] Mougel F, Debarbieux S, Ronger-Savlé S et al (2009) Methylaminolaevulinate photodynamic therapy in patients with multiple basal cell carcinomas in the setting of Gorlin-Goltz syndrome or after radiotherapy. Dermatology 219(2):138-142. https://doi.org/10.1159/000228316
[12] Girard C, Debu A, Bessis D et al (2013) Treatment of Gorlin syndrome (nevoid basal cell carcinoma syndrome) with methylaminolevulinate photodynamic therapy in seven patients, including two children: interest of tumescent anesthesia for pain control in children. Journal of the European Academy of Dermatology and Venereology: JEADV 27(2):e171-175. https://doi.org/10.1111/j.1468-3083.2012.04538.x
作者简介
通讯作者

吴丽莎,医学博士,硕士生导师。中南大学湘雅医院医学科学研究中心,副研究员。主要研究方向为皮肤银屑病发病机制及遗传易感性、皮肤黑素瘤发病机制研究。先后获得国家自然科学基金青年基金项目1项,面上项目2项,湖南省自然科学基金面上项目1项。发表SCI论文30余篇,其中以第一或通讯作者发表SCI论文18篇。先后获得湖南省科学技术二等奖、湖南省医学十大临床创新技术奖、全国妇幼健康科学技术二等奖、中南大学教学成果一等奖等。
第一作者

蒋梓汐,医学博士,毕业于中南大学湘雅医学院临床医学(八年制)专业,以第一作者身份发表SCI论文10篇,曾获“国家奖学金”、“中南大学优秀学生”、“中南大学优秀毕业生”等荣誉,就职于中山大学附属第一医院皮肤科。
第一作者

刘鑫,医学博士,毕业于中南大学湘雅医院,就职于空军军医大学西京医院皮肤科,以第一及通讯作者发表SCI论文5篇。
转载本文请联系原作者获取授权,同时请注明本文来自丁琛科学网博客。
链接地址:https://wap.sciencenet.cn/blog-3558836-1500329.html?mobile=1
收藏